"250mg ampicillin with visa, antimicrobial klebsiella".
By: Y. Rathgar, M.A., Ph.D.
Professor, University of Tennessee College of Medicine
The Circovirus has a common nine-nucleotide stemloop structure at its replication origin antibiotic resistance plasmid order 250 mg ampicillin with visa. The genome of Circovirus is ambisense antibiotics for acne breakout discount ampicillin 250 mg amex, as the largest Rep protein is coded by the genomic strand while the other two proteins are coded by the antigenomic strand (Figure 27 antibiotics for uti penicillin allergy buy ampicillin 250mg low price. Clockwise arrows: translations on the antigenomic strand; counterclockwise arrows: those on the genomic strand Okamoto et al virus 79 purchase ampicillin 250mg. However, it was not likely to constitute a complete genome because of the lack of a terminal repeat. However, the details of the biological significance of these motifs remained unclear, as no functional survey had been attempted. A single host can be infected with both virus groups, but there are some hosts with only one virus, indicating that the replications of these viruses are independent. Why and how these viruses can survive with such a wide spectrum of diversity is still unclear. Although the genomic sizes of these two viruses are very different, they share several common features. The structures of the coding regions in these two virus groups are also similar to each other. Although 2060% of patients with idiopathic fulminant hepatic failure (Charlton et al. Most reports suggest that there is no significant association with liver diseases such as chronic hepatitis or hepatocellular carcinoma (Cossart, 2000). Given this assumption, we calculated an expected protein size of 286 and 290 amino acids. However, because they intentionally deleted the region including the authentic initiation codon of the natural 1. The open triangle indicates the position of the cap site while the closed triangle indicates that of the polyA signal. The solid lines indicate exons, the dotted lines represent introns, and the boxes indicate coding regions. It is noteworthy that during the period covered by the two sets of recommendations more than 60 new virus diseases have been recognised in the human population (Figure 28. As with most emerging virus infections, these are examples of virus diseases that threaten public health throughout the world and are not limited in their potential geographic range. As pointed out in the first report on emerging infections, in the context of infectious diseases, there is nowhere in the world from which we are remote and no one from whom we are disconnected (Lederberg et al. Some of these are natural events that can be responded to , but not prevented from occurring, such as microbial adaptation and change, and climate and weather. Others are societal and political in origin and could be eliminated, such as the breakdown of public health measures, and poverty and social inequality. This chapter will consider the factors responsible for the emergence of new virus infections under four broad headings: (a) virus evolution; (b) human demographics, susceptibility to infection and behaviour; (c) improved technology for the detection of virus infection; and (d) increased contact with vectors of virus infection. By considering examples of virus emergence under each category, the factors responsible for the remarkable global increase in human virus infections over the last 15 years (Figure 28. For example, an outbreak of poliomyelitis in Hispaniola in 2001 was caused by a recombinant virus between the live Sabin poliovirus vaccine strain and an enterovirus, which restored the pathogenicity of the vaccine virus (Kew et al. Human Demographics, Susceptibility to Infection, and Behaviour Changes within the host population have contributed greatly to the emergence of virus diseases during the past 20 years. Increases in World Population and Global Travel the rapid increase in the world population has combined with the greatly enhanced opportunity for global travel to increase the opportunity for persons to come into contact with virus diseases formerly considered to be exotic to the developed world (such as Lassa fever, which causes 5000 deaths/year in West Africa). Although 102 people had contact with him in the Chicago hospital, fortunately none of these contacts became infected. Other cases were soon identified in Hanoi and in Hong Kong, and many of these were health care workers. In cases where two viruses of distinct genetic lineage infect the same cell, it is possible for exchange of genome segments to occur, giving rise to a new reassortant virus that may have altered properties of transmission or pathogenesis. Recombination the third most common mechanism of virus evolution is recombination between the genomes of two different viruses. Over the next few weeks it became clear that all these cases of severe respiratory disease could be linked to a hotel in Hong Kong (Hotel M), where the index case of the disease, a 65 year-old medical doctor from Guangdong Province in China, had arrived on 21 February.
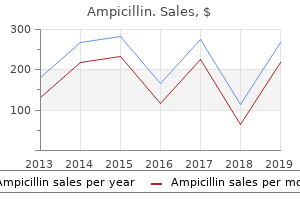
However virus yang menguntungkan generic 500 mg ampicillin with visa, in infections caused by non-polio enteroviruses there is almost always complete recovery from paresis antibiotic eye drops for dogs effective ampicillin 250mg. Coxsackie viruses of both group A and group B (especially types B1B6 antimicrobial ointment neosporin order ampicillin pills in toronto, A7 and A9) infection 7 weeks after dc discount ampicillin 500 mg mastercard, many echoviruses (notably types 4, 6, 11, 14, 16, 25, 30 and 31) as well as enterovirus 71 have been associated with aseptic meningitis. A pleocytosis, usually of the order of 10500/ mm73, mainly of lymphocytes is often, although not invariably present. During the first day or so after the onset of symptoms, polymorphonuclear leukocytes may predominate. Patients with hypogammaglobulinaemia may develop persistent infections following enterovirus infection, associated with chronic meningeal irritation, encephalitis, insidious intellectual impairment or, sometimes, a dermatomyositis-like syndrome (Wilfert et al. Many echoviruses and Coxsackie viruses B have been shown to cause such persistent infections; occasionally, multiple serotypes may be involved. Patients with hypogammaglobulinaemia may also develop paralytic disease following administration of attenuated live polio vaccine. Heart Disease Myocarditis A wide range of viruses may cause myocarditis, including ortho- and paramyoxoviruses, togaviruses, herpesviruses and adenoviruses. In addition, current understanding of pathogenesis in viral myocarditis derives mainly from studies of Coxsackie B virus infection, including both clinical studies in humans and experimental studies of Coxsackie B3 virus-induced murine myocarditis. Other enteroviruses, including polioviruses, Coxsackie A viruses and echoviruses, may also cause myocarditis, and the relative importance of other non-polio enteroviruses may have been underestimated in recent years because of the wider availability of serological tests for Coxsackie virus B infection. Diagnosis therefore requires histological examination of endomyocardial biopsy or autopsy tissue. Neonatal myocarditis can be rapidly fatal, and may be confused with congenital heart disease. In infants Encephalitis Although herpes simplex virus is the most commonly identified pathogen in patients with encephalitis (see Chapter 2A), enteroviruses are increasingly recognised as encephalitic agents (Modlin et al. Enteroviral encephalitis may be associated with aseptic meningitis, or may present with absent or minimal meningeal involvement. Although most patients recover uneventfully, a few have neurological sequelae or damage to the hypothalamicpituitary axis, which causes endocrine disturbance. Because myocarditis may present some time after the initiating viral infection, specific antibody titres may have already peaked. Thus, serological investigation using paired acute and convalescent samples may fail to demonstrate a diagnostic rise in titre. Enterovirus IgM testing may be used in the absence of suitably paired sera or isolation samples, but IgM seroprevalence in the community can be significant, especially during high-activity seasons, reflecting asymptomatic infection. Late in infection (911 days of illness) the size of the heart is increased, largely due to dilatation of the left, and occasionally the right, ventricle. Initially the inflammatory infiltrate is composed of polymorphonuclear leukocytes, but by day 5 or 6 mononuclear inflammatory cells are found. In contrast to the abrupt, severe and often fatal disease seen in the neonatal period, viral myocarditis in adolescents and adults usually has a delayed onset, often following an upper respiratory (typically influenza-like) or gastrointestinal illness. Acute heart disease may become evident a week to 10 days later and has a presentation that can mimic myocardial infarction, coronary artery occlusion or progressive heart failure. In a proportion the main presenting feature is pericarditis, characterised by acute, often severe, retrosternal chest pain. Other clinical findings include shortness of breath, tachycardia, arrhythmias, murmurs, rubs and cardiomegaly (due to ventricular dilatation or pericardial effusion). Death can supervene due to arrhythmias or congestive heart failure, but this is relatively uncommon. As in the neonatal infection, manifestations of systemic disease in adults may be noted. In Coxsackie virus B infections these may include pleurodynia, meningitis, hepatitis, orchitis, lymphadenopathy and splenomegaly. There may be recrudescences following the acute episode; up to 20% of patients in whom the major presenting feature is pericarditis will experience one or more relapsing episodes in the following months or years (Muir et al. Viral infection of the myocardium is believed to be a prerequisite to myocarditis, although antiviral cellular immune responses and autoreactive T cells activated following local tissue damage and release of sequestered autoantigen are likely to be important effectors of myocardial pathology (Horwitz et al. Thus, while steroid therapy has been used in patients with myocarditis, evidence of efficacy is lacking (Mason et al.
This chapter aims to provide the practical knowledge and approaches required to enable microbiologists and virologists to control the spread of virus infection in hospitals antibiotic used for acne ampicillin 250mg amex. Indeed virus united states department of justice buy ampicillin without a prescription, the entire subject of nosocomial virus infection has not had the prominence it deserves and has been a largely neglected area antibiotic before dental work discount ampicillin 500 mg with amex. This is surprising infection 1 buy ampicillin 250mg on line, as hospitals are a particularly easy target for several virus groups and may act as centres of virus amplification for the further spread of virus in the wider community. Global travel has also meant that increasingly the staff who work in health services come from all over the world. This brings with it other unique problems, such as increased susceptibility rates to chickenpox if staff are from equatorial climes. Very often virology is able only to prevent secondary cases where the incubation period is relatively long. Preventing the nosocomial spread of viral respiratory and gastrointestinal pathogens, however, with very short incubation periods of only hours to a few days, relies heavily on the staff admitting the patient recognising the potential for transmission and adhering strictly to basic infection control measures, such as hand-washing. The admission to single rooms of patients experiencing viral prodromes of, for example, parvovirus or measles during epidemic seasons or local upsurges, and cohort nursing are very effective but require thought from admitting teams. To facilitate this approach, clear, concise guidance from the virology, infection control and occupational health departments on how to manage individual virus infections and staff exposures to them is required. Although rapid diagnosis and excellent communication with staff in the clinical areas are essential if nosocomial infection is to be prevented, anticipating recurring problems. In this last chapter we cover the burden of nosocomial virus infection of the most important viruses. Section A discusses blood-borne viruses, whilst section B illustrates the problems, and some of the solutions to controlling the spread of viruses by all other routes and means of contact. Practical measures that should be taken to prevent an outbreak or limit its spread and guidance on the management of staff susceptible to particular agents are also given. Patient-to-patient transmission can also occur, usually only where there is a deficiency in infection control procedures. The risk of transmission for all three will depend to a large extent on the amount of virus inoculated, and this in turn will depend on the viral load in the source and the volume and type of body fluid transferred. More recently there have Principles and Practice of Clinical Virology, Fifth Edition. The aim of such protocols is to prevent, or at least control, exposure to hazardous substances. Only two nosocomial infections have been identified in two separate look-backs-one involving an orthopaedic surgeon in France and 1000 patients tested (Lot et al. Wash hands before and after contact with each patient, and before putting on and after using rubber gloves. Cover existing wounds, skin lesions and all breaks in exposed skin with waterproof dressings. Avoid sharps usage where possible, and where sharps usage is essential, exercise particular care in handling and disposal. Avoid wearing open footwear in situations where blood may be spilt, or where sharp instruments or needles are handled. Wear gloves when cleaning equipment prior to sterilisation or disinfection, when handling chemical disinfectant and when cleaning up spillages. Safe handling and disposal of sharps involves the adequate supply and positioning of sharps containers, the placing of all disposable sharps in such containers immediately after use, not overfilling such containers and avoiding resheathing needles, unless done by the single-handed technique with or without an appropriate device. Specific guidance for reducing the risk of percutaneous and mucocutaneous exposure during surgical procedures is also given in this document. Details are given in the national guidelines (Department of Health, 1997; Centers for Disease Control, 1998). Occupational health services are responsible for keeping accurate immunisation records for all employees and administering booster doses where appropriate. As mentioned previously, although the risks are small, such infections attract a disproportionate amount of media publicity. Close follow-up of exposed individuals is recommended with baseline and follow-up blood tests. Centers for Disease Control (1991) Recommendations for preventing transmission of human immunodeficiency virus and hepatitis B virus to patients during exposure prone invasive procedures.
Varimax-Rotated Factor Loadings of Questionnaires Across all Patients Component 1: Negative affectivity virus 78 purchase 250 mg ampicillin free shipping. Following varimax rotation (based on three unrotated factors with eigenvalues greater than 1) antibiotics for uti and bladder infections order genuine ampicillin on-line, the analysis resulted in three factors of (1) general distress/negative affectivity (k 5 6 antibiotic susceptibility testing cheap 500 mg ampicillin visa. Table 2 lists the factor loadings for individual questionnaires antibiotics for acne and rosacea buy cheap ampicillin 500 mg on line, which were consistently high (0. Interestingly, the questionnaires also loaded onto specific factors in a manner largely consistent with discriminable face validity. Linear trend tests were conducted for each of the mean factor scores across the defensive dimension. Figure 3B illustrates the mean negative affectivity factor scores for each group of patients arrayed along the defensive reactivity dimension. Only the broad distress/negative affectivity factor showed a reliable change that systematically increased from hyperresponders to hyporesponders (linear, F(1,420) 5 4. To adapt it for anxiety patients, the term illness is replaced by mental health problems. Interview Units of Analysis Thus far, the data suggest that a factor of broad distress/negative affectivity-including disorder-nonspecific and transdiagnostic functional impairment-is inversely related to defensive physiological reactivity during an emotional imagery challenge. Thus, reports of greater broad distress are related to lower levels of defensive activation, whereas more pronounced defensive mobilization is related to reports of less broad distress and impairment. Modest evidence suggested slightly higher aversiveness ratings for more reactive patients (compared to all other groups) that was specific to personal fear imagery (category, F(4,412) 5 5. As such, we have termed this nonspecific self-reported symptom array negative affectivity to highlight the influence of multiple pathologies in modulating defensive reflex physiology. We also found that cumulative life stressors and trauma exposure are related to blunted reactions. The latter specifically included subscales of stressors in the last 6 months and lifetime both weighted for stressor impact on well-being (Social Readjustment Rating 3. Supporting this, the proportion of patients diagnosed with either principal fear or anxious-misery disorders (N 5 238) differs in each of the five groups across the defensive dimension, v2(4) 5 20. As illustrated in Figure 3D, the proportion of patients diagnosed with principal anxious-misery disorders progressively increases when moving from the hyper- to the hyporesponsive end of the continuum, whereas the opposite is the case for patients with circumscribed fear disorders. Notably, while these data illustrate how patients diagnosed with circumscribed fear and anxious-misery disorders tend to show different defensive reactions, it is also critical to underscore the tremendous heterogeneity in the proportion of principal disorders in each quintile. In general, measures derived from the patient interview have not, so far, proved to vary significantly with the defensive reactivity dimension as it is defined psychophysiologically. The measures tested included the percentage of patients with/without (as well as the number of) comorbid anxiety or depressive disorders, clinician ratings of disorder severity and prognosis, and patient-reported disorder chronicity. Further analysis suggests that the failure to find these effects reflects, in part, the fact that a clinician makes judgments about a given patient relative to other patients with the same principal diagnosis. Thus, for example, the 91 patients in the current sample with the highest clinicianrated severity, transdiagnostic questionnaire measures of symptom intensity varied dramatically. Relatedly, when 59 (of the 425) patients whose prognosis was rated as "excellent" were rated, the subset of patients with specific phobia scored a mean of 6. Considering the large, multimeasure, multimethod nature of the data that investigators are likely to accumulate, many analytic strategies will need to be essayed. As our own anxiety research program developed, we became increasingly aware of the high variability within and between diagnoses and measures, and the need for ever larger samples. Very likely, we will soon be in the domain of "big data," and variations of more complex methodologies. The new analyses, however, point to systematic variations in the concordance between physiological measures, which now include both skin conductance and facial action. Furthermore, concordance is highest in the most reactive patients and palpably diminishes as negative affectivity increases across the defensive reactivity dimension. Notably, these different patterns of concordance do not emerge clearly when diagnostic category is used to define anxiety groups. It is still possible that certain phenotypes are marked by discordance in specific defensive measures during personal fear imagery. It will be useful in the future to consider within-participant data coherence as another dimension in exploring its relationship to other units of analysis. Imagery of standard survival fear scenes prompted palpable defense reactions that similarly decreased across the physiologi- P.
Severe (cephalic) tetanus non prescription antibiotics for acne discount ampicillin 250mg on-line, involving the cranial nerves antibiotics kinds buy discount ampicillin 250 mg on-line, is distinguished by its shorter incubation period antibiotics fragile x generic 250 mg ampicillin overnight delivery, the presence of trismus virus with headache discount ampicillin 250 mg online, the persistence of muscular rigidity between spasms and the absence of pleocytosis. Herpes simiae (B virus) encephalomyelitis, transmitted by monkey bites, has a much shorter incubation period than rabies (34 days). The diagnosis can be confirmed virologically and the patients treated with aciclovir. Clinical Diagnostic Methods in Human Rabies Haematological and Biochemical Tests Routine haematological and biochemical tests are initially normal, apart from neutrophil leukocytosis. The clinical features typical of rabies were the apparantly subjective parasthesiae of the bitten limb, the cardiac conduction defect (if it was a new finding) and the high antibody level. The rabies antibody response to nervous tissue vaccines are higher than usual in patients with severe post-vaccinal encephalitis (Hemachudha et al. After 20 days he developed a meningitic illness progressing to encephalitis, with unilateral weakness maximal in the bitten arm. Focal seizures, paralysis, cerebral oedema and coma ensued, lasting more than a week. Features suggesting rabies were the dominant signs in the bitten limb, a cardiac arrhythmia and the high antibody level. He had had preexposure prophylaxis with duck embryo rabies vaccine with a neutralising antibody titre of 1:32 6 months before exposure. A gradual improvement was followed by onset of a personality disorder and dementia. He improved over 3 weeks, and reacted to painful stimuli, but quadriplegia persisted, he became blind and deaf and eventually died after 2 years and 10 months. Minimal gadolinium enhancement, indicating mild inflammation, may be seen in the later stages of the clinical course. Similar changes in the spinal cord, suggestive of myelitis, might indicate a diagnosis of paralytic rabies. The non-specific changes reported to date would not be diagnostic of rabies infection. Recovery from Rabies Encephalitis Animals of several species have recovered from rabies (see above) and humans with paralytic rabies can survive for several weeks, especially with intensive care, but the illness progresses relentlessly. Five patients over the last 30 years have been claimed as survivors of encephalitis. Two of the patients were treated post-exposure with rabies vaccines of nervous tissue origin. In Argentina in 1972, a 45 year-old woman was bitten by her clinically rabid dog, began a course of suckling mouse brain vaccine 10 days later (Porras et al. Three weeks after the bite she had parasthesiae of the bitten arm, with tremors, myoclonic spasms, ataxia and other signs of cerebellar dysfunction. Clinical features included hypertonia, tetraparesis, dysphonia, dysphagia, varying levels of consciousness and a cardiac conduction defect, with slow resolution over a year. The wound was not cleaned but she was given purified chick embryo cell rabies vaccine (see section on Prophylaxis, below) on days 0, 3 and 7 after the bite. Sixteen days later she would not drink and developed fever, hallucinations and impaired consciousness, which progressed to coma with excessive salivation and focal seizures. After 3 months of coma, improvement began very slowly but after 18 months she had spasticity, tremors and involuntary limb movements. Neurological illnesses following human diploid cell rabies vaccine has been reported rarely (see below; Side Effects of Tissue Culture Vaccine) but have been relatively mild. Rabies virus was not isolated, nor was antigen identified, in these patients thought to have recovered from rabies, but false negative results may have been obtained because samples were taken late, when there was already a high titre of antibody neutralising the virus or covering the epitopes of the antigens. The diagnosis may remain in some doubt in those patients given vaccines of nervous tissue origin, as post-vaccinal encephalitis can produce similar signs and symptoms (Label and Batts, 1982). Severe impairment of nervous function was irreversible before the infection was controlled, presumably by the immune response.
Buy generic ampicillin 500mg online. New HIV Viral Load Testing Laboratory launched at KEMRI | KTN News Desk.





