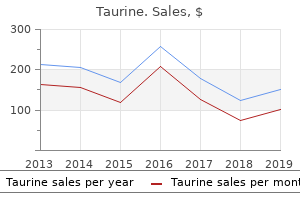
"Order taurine with a mastercard, administering medications 6th edition".
By: U. Cronos, M.A., M.D., M.P.H.
Co-Director, University of Kansas School of Medicine
A Cochrane review of randomized controlled trials using computerized advice to improve glucose control in the hospital found significant improvement in the percentage of time patients spent in the target glucose range medications 44334 white oblong order genuine taurine line, lower mean blood glucose levels medicine 5277 purchase cheap taurine, and no increase in hypoglycemia (10) symptoms 8 days after iui cost of taurine. Thus 7r medications order taurine australia, where feasible, there should be structured order sets that provide computerized advice for glucose control. Diabetes Care Providers in the Hospital Recommendation Even the best orders may not be carried out in a way that improves quality, nor are they automatically updated when new evidence arises. To this end, the Joint Commission has an accreditation program for the hospital care of diabetes (18), and the Society of Hospital Medicine has a workbook for program development (19). E Appropriately trained specialists or specialty teams may reduce length of stay, improve glycemic control, and improve outcomes, but studies are few (12,13). People with diabetes are known to have a higher risk of 30-day readmission following hospitalization. Specialized diabetes teams caring for patients with diabetes during their hospital stay can improve readmission rates and lower cost of care (15,16). Blood glucose levels that are persistently above this level may require alterations in diet or a change in medications that cause hyperglycemia. Level 1 hypoglycemia in hospitalized patients is defined as a measurable glucose concentration,70 mg/dL (3. Recent randomized controlled studies and metaanalyses in surgical patients have also reported that targeting perioperative blood glucose levels to ,180 mg/dL (10mmol/L) is associated with lower rates of mortality and stroke compared with a target glucose,200 mg/dL (11. Insulin therapy should be initiated for treatment of persistent hyperglycemia starting at a threshold $180 mg/dL (10. Conversely, higher glucose ranges may be acceptable in terminally ill patients, Table 15. Intravenous insulin infusions should be administered based on validated written or computerized protocols that allow for predefined adjustments in the infusion rate, accounting for glycemic fluctuations and insulin dose (2). Noncritical Care Setting In the patient who is eating meals, glucose monitoring should be performed before meals. More frequent blood glucose testing ranging from every 30 min to every 2 h is required for patients receiving intravenous insulin. Observational studies have shown that safety standards should be established for blood glucose monitoring that prohibit the sharing of fingerstick lancing devices, lancets, and needles (25). Significant discrepancies between capillary, venous, and arterial plasma samples have been observed in patients with low or high hemoglobin concentrations and with hypoperfusion. An insulin regimen with basal, prandial, and correction components is the preferred treatment for noncritically ill hospitalized patients with good nutritional intake. A In most instances in the hospital setting, insulin is the preferred treatment for hyperglycemia (2). However, in certain circumstances, it may be appropriate to continue home regimens including oral antihyperglycemic medications (32). Regimens using insulin analogs and human insulin result in similar glycemic control in the hospital setting (37). If oral intake is poor, a safer procedure is to administer the rapid-acting insulin immediately after the patient eats or to count the carbohydrates and cover the amount ingested (37). A randomized controlled trial has shown that basal-bolus treatment improved glycemic control and reduced hospital complications compared with sliding scale insulin in general surgery patients with type 2 diabetes (38). Prolonged sole use of sliding scale insulin in the inpatient hospital setting is strongly discouraged (2,14). Therefore, premixed insulin regimens are not routinely recommended for in-hospital use. S176 Diabetes Care in the Hospital Diabetes Care Volume 42, Supplement 1, January 2019 Type 1 Diabetes For patients with type 1 diabetes, dosing insulin based solely on premeal glucose levels does not account for basal insulin requirements or caloric intake, increasing both hypoglycemia and hyperglycemia risks. Typically, basal insulin dosing schemes are based on body weight, with some evidence that patients with renal insufficiency should be treated with lower doses (41).
Food and Drug Administration requires that Nutrition Facts labels portray the trans fat content of packaged food symptoms gerd buy taurine 1000 mg fast delivery. Some municipalities 4 medications at walmart buy taurine us, such as New York City medicine 1700s buy discount taurine 1000 mg online, have banned the use of trans fats in restaurants medications used for anxiety buy taurine without a prescription. However, because of the potential dangers of alcohol abuse, health professionals are reluctant to recommend increased alcohol consumption to their patients. Red wine may provide cardioprotective benefits in addition to those resulting from its alcohol content (for example, red wine contains phenolic compounds that inhibit lipoprotein oxidation; see p. Although caloric intake in the United States has shown a modest increase since 1971, the incidence of obesity has dramatically increased (see p. During this same period, carbohydrate consumption has significantly increased (as fat consumption decreased), leading some observers to link obesity with carbohydrate consumption. However, obesity has also been related to increasingly inactive lifestyles and to calorie-dense foods served in expanded portion size. Classification of carbohydrates Dietary carbohydrates are classified as simple sugars (monosaccharides and disaccharides), complex sugars (polysaccharides), and fiber. Monosaccharides: Glucose and fructose are the principal monosaccharides found in food. Free fructose is found together with free glucose and sucrose in honey and fruits (for example, apples). Disaccharides: the most abundant disaccharides are sucrose (glucose + fructose), lactose (glucose + galactose), and maltose (glucose + glucose). Polysaccharides: Complex carbohydrates are polysaccharides (most often polymers of glucose) that do not have a sweet taste. Starch is an example of a complex carbohydrate that is found in abundance in plants. Common sources include wheat and other grains, potatoes, dried peas and beans, and vegetables. Fiber: Dietary fiber is defined as the nondigestible, nonstarch carbohydrates and lignin (a noncarbohydrate polymer of aromatic alcohols) present intact in plants. Soluble fiber is the edible parts of plants that is resistant to digestion and absorption in the human small intestine but is completely or partially fermented by bacteria to short-chain fatty acids in the large intestine. This delayed emptying also results in reduced peaks of blood glucose following a meal. Also, fiber-rich diets decrease the risk for constipation, hemorrhoids, and diverticulosis. Dietary carbohydrate and blood glucose Some carbohydrate-containing foods produce a rapid rise followed by a steep fall in blood glucose concentration, whereas others result in a gradual rise followed by a slow decline. Requirements for carbohydrate Carbohydrates are not essential nutrients, because the carbon skeletons of most amino acids can be converted into glucose (see p. However, the absence of dietary carbohydrate leads to ketone body production (see p. It is recommended that added sugar represent no more than 25% of total energy because of concerns that sugar may displace nutrient-rich foods from the diet, potentially leading to deficiencies of certain micronutrients. Simple sugars and disease There is no direct evidence that the consumption of simple sugars is harmful. Contrary to folklore, diets high in sucrose do not lead to diabetes or hypoglycemia. They yield 4 kcal/g (the same as protein and less than one half that of fat; see Figure 27. However, there is an association between sucrose consumption and dental caries, particularly in the absence of fluoride treatment. Nine of the 20 amino acids needed for the synthesis of body proteins are essential (that is, they cannot be synthesized in humans).
Mutation rates and founder effects act along with genetic drift to make certain genetic diseases more common (or rarer) in small medicine 2632 proven 1000mg taurine, isolated populations than in the world at large medications causing thrombocytopenia order 1000mg taurine otc. Genetic drift may then change allele frequencies and a new Hardy-Weinberg equilibrium is reached symptoms 3 weeks pregnant taurine 1000 mg with visa. Because of gene flow symptoms strep throat buy taurine 1000mg low price, populations located close to one another often tend to have similar gene frequencies. Gene flow can also cause gene frequencies to change through time: the frequency of sickle cell disease is lower in African Americans in part because of gene flow from other sectors of the U. Behavioral Science/Social Sciences Note Consanguineous matings are more likely to produce offspring affected with recessive diseases because individuals who share common ancestors are more liable to share disease-causing mutations. Consanguinity and Its Health Consequences Consanguinity refers to the mating of individuals who are related to one another (typically, a union is considered to be consanguineous if it occurs between individuals related at the second-cousin level or closer). Because of their mutual descent from common ancestors, relatives are more likely to share the same disease-causing genes. A Pedigree Illustrating Consanguinity Consequently, there is an increased risk of genetic disease in the offspring of consanguineous matings. These studies show that the offspring of first-cousin matings are approximately twice as likely to present with a genetic disease as are the offspring of unrelated matings. A population has been assayed for a 4-allele polymorphism, and the following genotype counts have been obtained: Genotype 1,1 1,3 1,4 2,3 2,4 3,3 3,4 4,4 Count 4 8 3 5 9 4 6 11 On the basis of these genotype counts, what are the gene frequencies of alleles 1 and 2 Genotype frequencies can be estimated from allele frequencies, but the reverse is not true. Once a population deviates from Hardy-Weinberg equilibrium, it takes many generations to return to equilibrium. The frequency of heterozygous carriers of an autosomal recessive mutation can be estimated if one knows the incidence of affected homozygotes in the population. In a genetic counseling session, a healthy couple has revealed that they are first cousins and that they are concerned about health risks for their offspring. The couple has an increased risk of producing a child with an autosomal dominant disease. The couple has an increased risk of producing a child with an autosomal recessive disease. If the incidence of cystic fibrosis is 1/2,500 among a population of Europeans, what is the predicted incidence of heterozygous carriers of a cystic fibrosis mutation in this population Phenotypic expression is variable and ranges from high urinary excretion of proline to neurologic manifestations including seizures. The incidence of Duchenne muscular dystrophy in North America is about 1/3,000 males. On the basis for this figure, what is the gene frequency of this X-linked recessive mutation The denominator of the gene frequency is 100, which is obtained by adding the number of genotyped individuals (50) and multiplying by 2 (because each individual has two alleles at the locus). These 2 genotypes yield 5 and 9 copies of allele 2, respectively, for a frequency of 14/100 = 0. Using the Hardy-Weinberg equilibrium relationship between gene frequency and genotype frequency, the gene frequency can then be used to estimate the frequency of the heterozygous genotype in the population. Only one generation of random mating is required to return a population to equilibrium (choice D). Because both members of the couple are healthy, neither one is likely to harbor a dominant disease-causing mutation (choice B). In addition, consanguinity itself does not elevate the probability of producing a child with a dominant disease because only one copy of the diseasecausing allele is needed to cause the disease. When it is transmitted by an affected female, it acts like a dominant mutation and thus would not be affected by consanguinity. Empirical studies indicate that the risk of genetic disease in the offspring of first cousin couples is approximately double that of the general population (choice E). The frequency of sickle cell disease is elevated in many African populations because heterozygous carriers of the sickle cell mutation are resistant to malarial infection but do not develop sickle cell disease, which is autosomal recessive.
It is not wholly new treatment spinal stenosis purchase line taurine, since opioid addiction and the resulting societal disruption have been major problems in many countries for hundreds of years treatment wasp stings buy taurine 1000 mg with mastercard, but its magnitude has increased exponentially in the past decades symptoms to diagnosis generic taurine 1000mg with mastercard. As this Consensus Study Report articulates medicine 81 generic 1000mg taurine visa, modern medicine and the science that underpins it have developed and provided a set of highly effective tools that can help address the opioid epidemic-specifically, three U. Most of the factors impeding their full use can and must be dealt with if real progress is to be made. These factors include the misunderstandings and stigma surrounding both addiction and the medications used to treat it as well as counterproductive ideologies that consider addiction simply a failure of will or a moral weakness, as opposed to understanding opioid use disorder as a chronic disease of the brain that requires medical treatment. Fortunately, there is a robust research enterprise that is continuing to work on opioid use disorder and its treatment. Knowledge needs include refining in detail the most effective protocols for administering medications to specific individuals and subpopulations and the identification of additional molecular targets and approaches to enable the development of new and even more effective medications. These brain changes-and the resulting addiction- can be treated with life-saving medications, but those medications are not available to most of the people who need them. Methadone, buprenorphine, and extended-release naltrexone are safe and highly effective medications that are already approved by the U. These medications also help people restore their functionality, improve their quality of life, and reintegrate into their families and communities. Withholding them on ideological or other non-evidencebased grounds is denying people needed medical care. However, some addiction treatment facilities that ban medications are still being supported by funding streams that are tied to the criminal justice system or housing authorities, creating strong incentives to steer patients toward non-medication-based treatment approaches. Building on decades of research, the scientific community has coalesced around the brain disease model of addiction. The evidence shows that these brain changes can be treated effectively with medications that help people refrain from using drugs, thus sharply reducing their risks of overdose and death. Patients who receive medication have higher treatment retention rates, better long-term treatment outcomes, and improved social functioning; they are also less likely to inject drugs or transmit infectious diseases. Methadone, buprenorphine, and extended-release naltrexone all work by targeting the mu-opioid receptor within the opioid system. Because each medication has a distinct mechanism of action, the most appropriate medication and dosage varies across patients and may vary in the same patient over the course of treatment. The existing medications are very effective, but they are not perfect; for example, evidence gaps remain about how to choose the most effective medication for a particular patient and how best to retain people in treatment, which is itself a significant problem. Even among patients who would benefit from the addition of behavioral interventions, it is better for them to receive medication with appropriate medical management than to have it withheld. The life-saving aspects of these medications have been established even in the absence of accompanying behavioral interventions. Given the resource limitations faced in many settings, it is critical that providers do not withhold medications from their patients just because behavioral interventions are not available. Unlike methadone, buprenorphine is approved to be prescribed in office-based settings, but only by providers who undergo specialized training and obtain a waiver from the Drug Enforcement Administration. Medications for Opioid Use Disorder Save Lives 1 1 Introduction the United States is facing an epidemic of opioid-related mortality and morbidity that is unparalleled in its scope and staggering in its impact. Drug overdoses are the leading cause of accidental deaths in the United States (Volkow et al. According to 2016 data from the National Survey on Drug Use and Health, more than 11. People who misuse prescription opioids are almost 20 times more likely to use heroin for the first time, and, although just 4 to 6 percent of people who misuse prescription opioids transition to heroin within 5 years, 80 percent of people who use heroin have previously misused prescribed opioids (Carlson et al. Heroin 1 Around two-thirds of people who misuse opioids report doing so for pain management; more than one-third of people who misuse opioids report obtaining them by prescription from a health care provider. Synthetic-opioid overdose deaths increased by 45 percent between 2016 and 2017 (Hedegaard et al. The impact of the opioid epidemic extends far beyond overdose mortality or the immediate consequences to individuals who use opioids or their families. Medication is also a core component of medically supervised withdrawal from opioids, as it can alleviate acute withdrawal symptoms and reduce cravings. Methadone and buprenorphine are known to be effective in relieving withdrawal symptoms during the acute phase of treatment (medically supervised withdrawal) and in reducing cravings and illicit opioid use when used for the long-term (known as the maintenance phase). Methadone is typically taken orally once daily and administered in person at opioid treatment programs.
The land-poverty crisis created an entire cohort of males into their thirties with no family responsibilities and 94 medications that can cause glaucoma cheap taurine 1000mg, often treatment of ringworm purchase taurine visa, no work and little hope medications breastfeeding order taurine 1000 mg on-line. Since most Rwandans were Hutu and most Hutu were rural dwellers medications knowledge generic taurine 1000 mg visa, most of the young men in these circumstances were naturally Hutu as well. As in every age and every part of the globe, such rootless young men turn into big trouble looking for the right opportunity; they are made-to-order recruits for possible violence. Lacking all conviction, these are the young men who become mercenaries and paid killers for whichever side grabs them first. The new political parties rushed to take advantage of this convenient pool of idle, bored males for their militias or youth wings. There seems to us an obvious lesson in this analysis for the international financial institutions. There is no such thing as an economic programme that is purely neutral and has no political or social impact. Yet even they consider it "irresponsible in the extreme" for the international financial institutions to have ignored the overall circumstances of Rwanda at the time. Thus, important opportunities to use aid to induce a response away from increasingly violent conflict through the strategic use of incentives and disincentives were missed. At the same time, aid increased significantly as the rich world came to the rescue of one of its favourite aid destinations, and certain traditional truths about the aid enterprise remained the rule. Probably more than two-thirds of all project costs everywhere go to fund the salaries of foreign experts, the construction of project infrastructures, and vehicles. Most development aid, in other words, ends up in the hands of the richest one per cent of people in society, those for whom it is least intended. As one student of development aid in rural Rwanda put it, as far as farmers are concerned, most projects "benefit only those who promote them and those who work for them. They are refusing to listen to the burgomaster and even lock him out of his office or block the road so he cannot get there. The military dictatorship frustrated the ambitions of many within the Rwandan elite. Pressure for democratization from both within and outside the country forced Habyarimana to accept multiparty politics. New formations created new sources of intra-elite tensions, while the small clique of north-western Hutu who dominated the organs of state grew increasingly anxious about losing their control and dominance in the state and its institutions. The favouritism they showed towards their old regional loyalties, always a characteristic of the Habyarimana years, became increasingly flagrant. Whether in terms of educational places, government work, or aid projects, the northern regions derived benefits from government policies out of all proportion to their population. Many observers were well aware of the greed of the Akazu and did not doubt their fanatical determination to maintain their privileges. But, as members of this Panel can understand perfectly well, few could even contemplate the lengths they would go to do so. For the rest of the political class, regional grievances were at the heart of most discontent. Non-northerners wanted a larger share of government positions, but Rwandan leaders were too clever to be caught fighting publicly over their own enrichment. Soon the Akazu was using the tried-and-true ethnic card to divert attention away from differences among the Hutu. Meanwhile, the frustrated Hutu outsiders discovered that democracy was an appealing battle cry and one cheered on by westerners who had rediscovered the virtues of democracy for poorer countries when the Cold War ended. The majority of people watched the new competition among elites with growing alienation, since none of it seemed to have any connection with their lives. What rural Rwandans wanted was not more self-seeking politicians, but policies and programmes to alleviate their severe distress. What they got from their leaders was a proliferation of largely irrelevant new political groups and the insistence that the real predicament was the treachery of their Tutsi neighbours. The most significant consequences of the so-called democratization movement were profoundly unintended: the movement ended up inciting malevolent forces within society while alienating even further the majority of the population. Once again, Rwandans confounded those who persisted in seeing them as almost mindlessly obedient to authority. Anti-government demonstrations and strikes were held in 1990, and even the Catholic church felt obligated to express publicly its dissatisfaction with government policies. On the other hand, with only a few laudable exceptions, it must be recorded that the leadership of church and state remained tightly bound throughout these eventful years, earning the former the nickname in anti-government circles of "the Church of Silence.
Purchase generic taurine pills. aids symptoms.





